
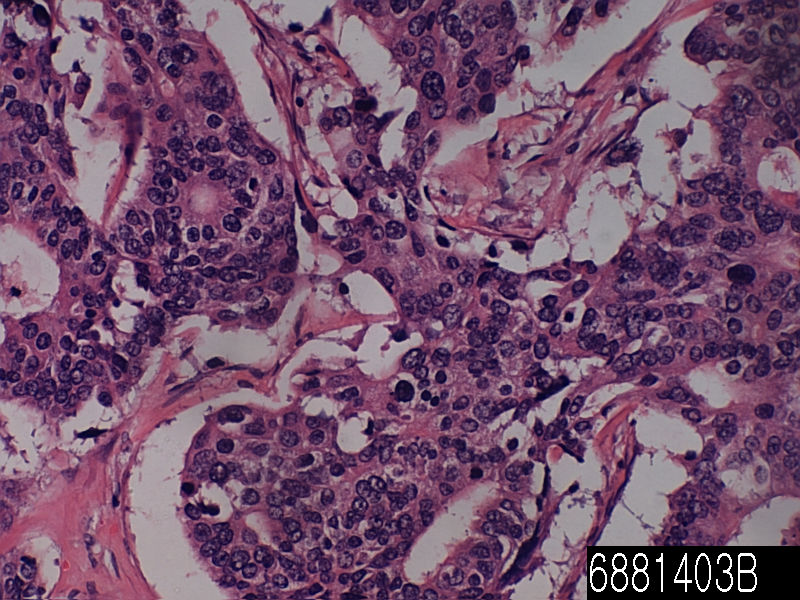
| Product name | Rectum adenocarcinoma MD |
| Cat. No. | 6881403B |
| No. of samples | 1 |
| Description | rectum adenocarcinoma MD Age/Sex : 63/F |
| Price | 197 EUR |
| 260 USD | |
| 170 GBP |
Product Related Literature
The rectoprostatic fascia is a membranous partition in the lowest part of rectovesical bag. This split of the prostate and bladder of the rectum. It consists of a fibromuscular structure with several layers, which are fused together and cover the seminal vesicles. It is also called fascia Denonvilliers “, after French anatomist and surgeon Charles-Pierre Denonvilliers. Structure corresponds had rectovaginal fascia in women. At postoperative transsexual women, the vaginal cavity created by him. Rectoprostatic in the rear bumper also inhibits proliferation of prostate adenocarcinoma due to the invasion of the rectum is more often than is the invasion of other adjacent structures.
The objectives of the follow-up are to be diagnosed at an early stage or metastasis or tumors that develop later, but did not originate from the original cancer. The U.S. National Comprehensive Cancer Network and American Society of Clinical Oncology provide guidelines for the monitoring of colorectal cancer. A medical history and physical examination is recommended every 3 to 6 months for 2 years, and then every 6 months for 5 years. Carcinoembryonic antigen blood measurements follow the same time, but it is recommended only in patients with T2 or more lesions, which are candidates for intervention. A CT-scan of the chest, abdomen and pelvis can be considered for the first year, 3 years for patients who are at high risk of relapse (e.g., patients who are poorly differentiated tumors or venous or lymphatic invasion) and are candidates for therapeutic operation (to be treated). Colonoscopy can be done after one year unless it can be done during the initial braking by preventing mass, in which case it should be performed after 3 to 6 months. If villous polyp, a polyp> 1 centimeter or high grade dysplasia is found, it can be repeated after 3 years, then every 5 years. For other offenses, a colonoscopy can be repeated after 1 year. Routine PET scan or ultrasound, chest X-ray, complete blood count and liver function tests is not recommended. These guidelines are based on recent meta-analyzes showing intensive surveillance and close follow-up can reduce the 5-year mortality rate from 37% to 30%.
Cytopathology is a branch of pathology that studies and diagnoses diseases on the cellular level. Discipline was founded by Rudolf Virchow in 1858. A common application of Cytopathology a smear is used as a screening tool for the detection of pre-cancerous cervical lesions, and the prevention of cervical cancer. Cytopathology is also commonly used in the investigation of thyroid disorders disorders including sterile body cavities (peritoneal, pleural and cerebrospinal), and a wide range of other body sites. It is commonly used to aid in the diagnosis of cancer, but it also helps in the diagnosis of certain infectious diseases, and other inflammatory conditions. Cytopathology typically used for samples of the free cells or tissue fragments, in contrast to histopathology and studies whole tissues. Cytopathologic tests are sometimes called smear tests because samples can be smeared on a glass microscope slide for subsequent staining and microscopic examination. However, sputum samples can be prepared in other ways, including cytocentrifugation. Miscellaneous Pap tests may be used for diagnosis of cancer. In this sense, it is called cytology smear. Cytopathology is often less accurately called cytology, which means “the study of cells.”
Various normal function of cell growth, metabolism, and division may fail or operate in unusual ways and cause disease. Cytopathology is best used as one of the three instruments, the second and third are physical examination and medical imaging. Cytology can not be used to diagnose the condition of the patient and the replacement operation, to obtain a larger sample. An example is the thyroid FNA; many benign conditions can be diagnosed with superficial biopsy and the patient can return to normal activities immediately. If the malignant disease is diagnosed, the patient may be able to launch the radiation / chemotherapy, or it can have an operation to remove and / or stage of the cancer. Some tumors may be difficult to biopsy as sarcomas. Other rare tumors my be dangerous to biopsy as pheochromocytoma. In general, fine-needle aspiration can be done anywhere, it’s safe to put the needle, including liver, lung, kidney, and superficial masses. Many doctors are not trained to perform fine-needle aspiration biopsies correctly and then when they do not get diagnostic material believe that cytology is not useful. Proper technique takes time to master. Cytotechnologists and cytopathologists can help doctors by going to the procedures and assist with collection techniques. A “speed reading” is a look under the microscope and tell your doctor if sufficient diagnostic material is obtained. Sputum samples must be well prepared, so that the cells are not damaged. Sometimes more information about the model is helpful. Immunohistochemical staining and molecular testing may be performed, particularly if the sample was obtained using a liquid-based cytology. Often the “Reflex” test is performed, such as HPV testing of an abnormal Pap test, or flow cytometry of lymphoma model.