
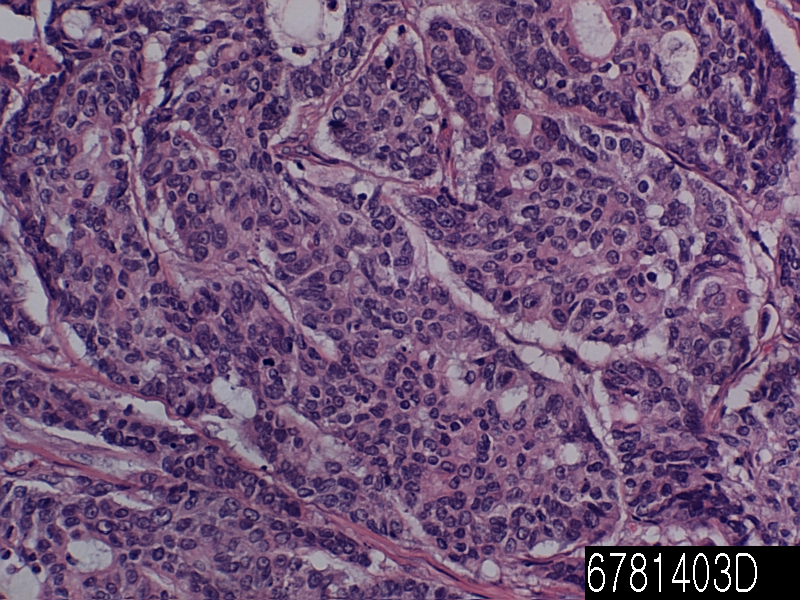
| Product name | Colon adenocarcinoma mucinous |
| Cat. No. | 6781403D |
| No. of samples | 1 |
| Description | colon adenocarcinoma mucinous Age/Sex : 44/M |
| Price | 197 EUR |
| 260 USD | |
| 170 GBP |
Product Related Literature
Mucinous cyst adenoma is a type of unification of tumor cyst adenoma. To those associated with invasive cancer, those not associated with invasive cancer – pathologist classifies intraductal papillary mucinous tumors (IPMNs) into two main groups. This separation is an important prognostic significance. Patients with intraductal papillary mucinous tumors are surgically removed that are associated with invasive cancer while have a poor prognosis, patients with surgical resection intraductal papillary mucinous tumor without invasive cancer related, I have an excellent prognosis. Intraductal papillary mucinous tumor without invasive cancer and the corresponding can be sub-categories into three groups further. They are IPMN and IPMN with high-grade dysplasia, and IPMN, dysplasia of low-grade, and moderate dysplasia. Since it is believed to be shifted from moderate dysplasia IPMNs, high-grade dysplasia or low-grade dysplasia, this classification, it is more important than isolation of cancer IPMNs connected by IPMNs each without invasive cancer it is but, IPMN is useful classification is associated with invasive cancer.
Intraductal papillary mucinous tumors, can come to the attention of the clinical in a variety of ways. Abdominal pain, nausea, the most common symptom is vomiting. (Skin and eyes caused by obstruction of the bile duct become yellow) jaundice patients with the most common symptoms to come to medical attention, weight loss, and there is acute pancreatitis them. That it is to establish the diagnosis more difficult, the signs and symptoms of these are not specific for internal papillary mucinous tumor. Therefore, in many cases, the doctor tells the additional checks. If you have any reason to believe that it may patient has internal papillary mucinous tumors, he or she, the physician can confirm that suspicion by using one of the imaging techniques. These include (MRCP) (EUS), magnetic resonance cholangiopancreatography computed tomography (CT), endoscopic ultrasound. These tests, to clarify the expansion of one of the branches of the pancreatic duct or pancreatic duct. In some cases, fine needle aspiration (FNA) biopsy can be obtained to confirm the diagnosis. Fine needle aspiration biopsy can be performed through the skin using a needle guided by computed tomography or ultrasound that is performed through the endoscope in the endoscopic ultrasound examination, or can.
(Small space or cavity) IPMN cysts of the pancreas. These cysts is seen in CT (X-ray computed tomography). However, many pancreatic cysts are benign (see the disease of the pancreas). Before developing the (asymptomatic patients) symptoms, increase in number of patients are diagnosed They are now. Another reason, when it is scanned in the (X-ray), in these cases, (incidentally) patients discovered accidentally damaged pancreas. I will be done to treat the IPMNs occasionally to 6% of patients who underwent pancreatic resection.
Scientists Sol Goldman Pancreatic Cancer Research Center reported in the 20 issue July Science Translational Medicine at the Johns Hopkins University, they are genes that can be used to distinguish harmless from gun cysts of the pancreas I developed a test based. Test might help you avoid surgery patient harmless cyst is unnecessary. And his colleagues Bart Vogel, was found to be (intraductal papillary mucinous tumor) has a mutation in the gene of GNAS GNAS and / or pre-cancerous cyst almost all of the pancreas. Researchers have tested a total of 132 intraductal papillary mucinous tumors for mutations in GNAS and KRAS. Almost all was or both mutation, of GNAS of KRAS. Harmless cysts and serous cyst adenoma as had KRAS mutations or GNAS, researchers then feel safe. Before it is possible to provide wide genetic testing, many patients should be tested further.
Thus, treatments of choice for the main channel IPMNs resection is the probability of approximately 50% of malignant tumors. Side branch IPMNs can be seen on a regular basis by the MRI or CT, but sometimes, cut at a rate of 30% of malignant tumors in the resection of these tumors eventually. About 80% in malignant, there was no 85% of the malignant disease survival after resection of IPMN five years, lymph nodes, and there is no circulation at all and 0% growth of malignant lymph nodes. It may include to move the body and tail of the pancreas removed whole or pancreas (pancreatic tail) of the (total pancreatectomy) below, to remove the head of the pancreas (pancreaticoduodenectomy). In some cases, surgery may be performed using minimally invasive techniques such as robotic surgery or laparoscopy.